Single- versus double-layer closure of the caesarean (uterine
Background Double-layer compared to single-layer closure of the uterus after a caesarean section (CS) leads to a thicker myometrial layer at the site of the CS scar, also called residual myometrium thickness (RMT). It possibly decreases the development of a niche, which is an interruption of the myometrium at the site of the uterine scar. Thin RMT and a niche are associated with gynaecological symptoms, obstetric complications in a subsequent pregnancy and delivery and possibly with subfertility. Methods Women undergoing a first CS regardless of the gestational age will be asked to participate in this multicentre, double blinded randomised controlled trial (RCT). They will be randomised to single-layer closure or double-layer closure of the uterine incision. Single-layer closure (control group) is performed with a continuous running, unlocked suture, with or without endometrial saving technique. Double-layer closure (intervention group) is performed with the first layer in a continuous unlocked suture including the endometrial layer and the second layer is also continuous unlocked and imbricates the first. The primary outcome is the reported number of days with postmenstrual spotting during one menstrual cycle nine months after CS. Secondary outcomes include surgical data, ultrasound evaluation at three months, menstrual pattern, dysmenorrhea, quality of life, and sexual function at nine months. Structured transvaginal ultrasound (TVUS) evaluation is performed to assess the uterine scar and if necessary saline infusion sonohysterography (SIS) or gel instillation sonohysterography (GIS) will be added to the examination. Women and ultrasound examiners will be blinded for allocation. Reproductive outcomes at three years follow-up including fertility, mode of delivery and complications in subsequent deliveries will be studied as well. Analyses will be performed by intention to treat. 2290 women have to be randomised to show a reduction of 15% in the mean number of spotting days. Additionally, a cost-effectiveness analysis will be performed from a societal perspective. Discussion This RCT will provide insight in the outcomes of single- compared to double-layer closure technique after CS, including postmenstrual spotting and subfertility in relation to niche development measured by ultrasound. Trial registration Dutch Trial Register ( NTR5480 ). Registered 29 October 2015.

Caesarean Section

PDF) Effect of single-versus double-layer uterine closure during caesarean section on postmenstrual spotting (2Close): multicentre, double-blind, randomised controlled superiority trial
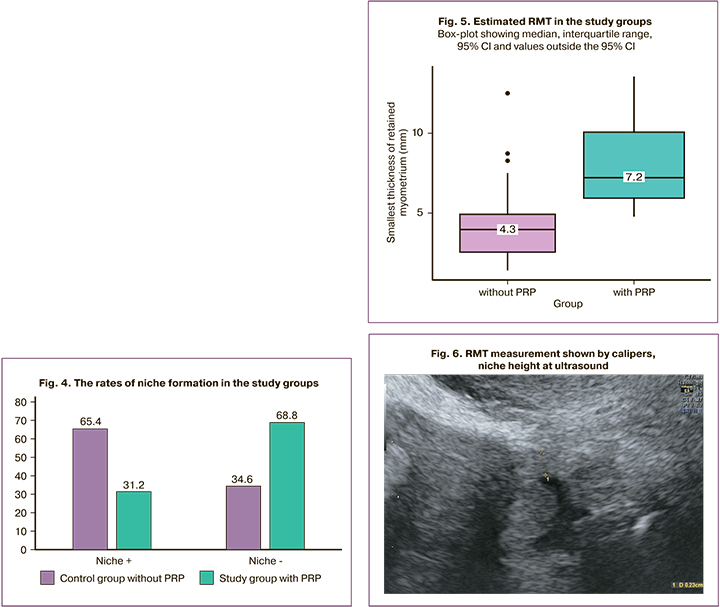
Ultrasound criteria of uterine scar secondary to placenta accreta spectrum metroplasty and use of platelet-rich plasma » Obstetrics and Gynecology

PDF) Hysteroscopic management of a uterine caesarean scar defect (niche) in women with postmenstrual spotting: a randomised controlled trial

Technical aspects of the laparoscopic niche resection, a step-by-step tutorial.

Why do niches develop in Caesarean uterine scars? Hypotheses on the aetiology of niche development. - Abstract - Europe PMC

PDF) Caesarean Section

Gynecological and postpartum ultrasonography of cesarean uterine scar defects: a pictorial essay

Technical aspects of the laparoscopic niche resection, a step-by-step tutorial.

Can uterine niche be prevented? - ScienceDirect
PDF) Effect of single‐ versus double‐layer uterine closure during caesarean section on postmenstrual spotting (2Close): multicentre, double‐blind, randomised controlled superiority trial

PDF) Morphological estimation of incomplete uterine scar rupture (dehiscence) in post- cesarean deliveries. Immunohistochemical studies

Why do niches develop in Caesarean uterine scars? Hypotheses on the aetiology of niche development. - Abstract - Europe PMC

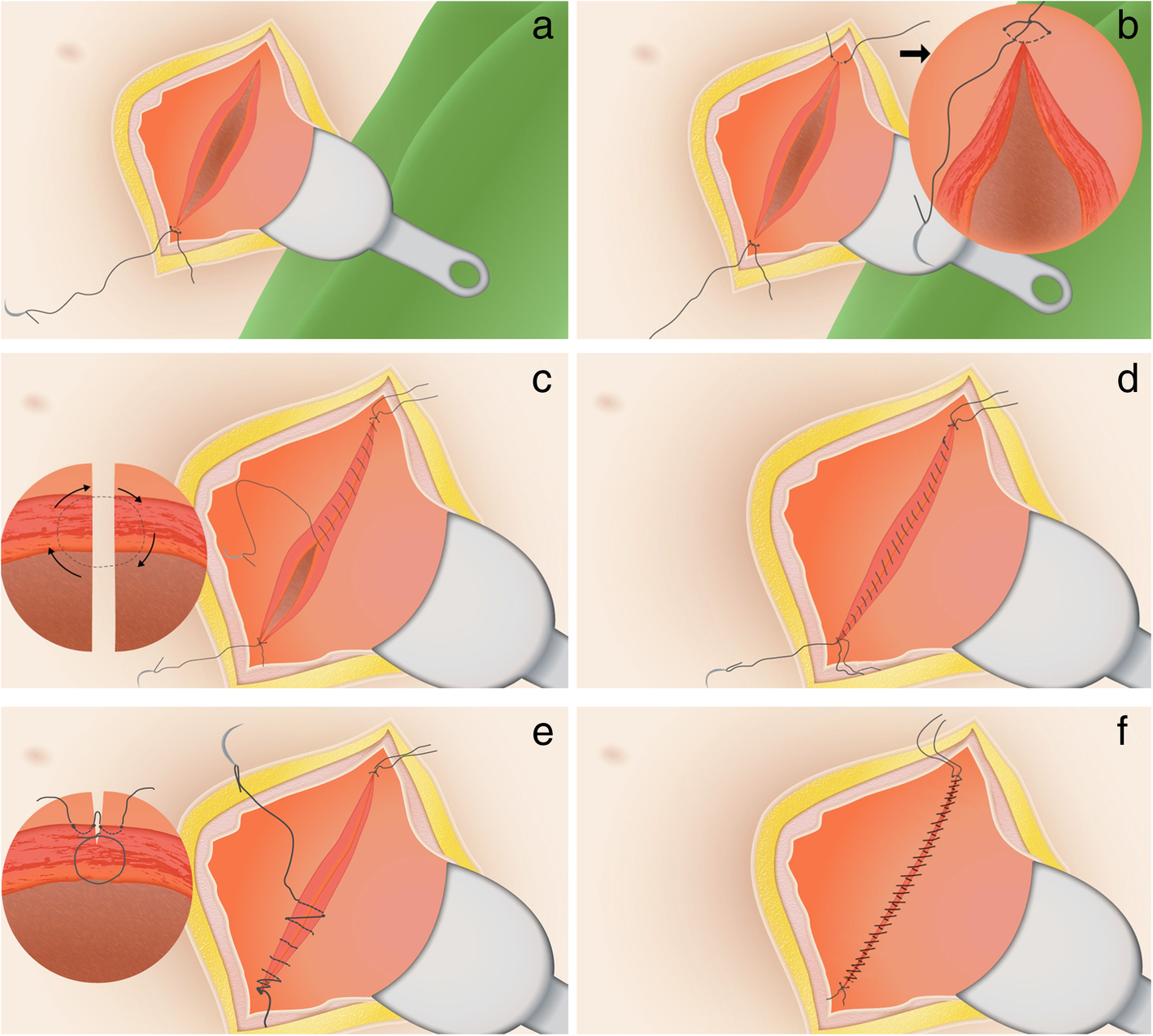
Double-layer uterine closure technique. a. Step 1: lateral suture; b.